
 Cardionerds: A Cardiology Podcast
Cardionerds: A Cardiology Podcast 275. Case Report: A Rare Cause Of Fatigue, Dyspnea, And Weight Loss In An Elderly Man – Brigham and Women’s Hospital
CardioNerds (Amit and Dan) join Dr. Khaled Abdelrahman, Dr. Gurleen Kaur, and Dr. Danny Pipilas from the Brigham and Women’s Hospital Residency Program for Italian food and cannolis at the North End in Boston as they discuss the case of an elderly man with primary cardiac lymphoma. They review an approach to intracardiac masses, discuss advantages and disadvantages of various imaging modalities for the evaluation of intracardiac masses, and also delve into anthracycline toxicity. The E-CPR segment is provided by Dr. Ron Blankstein, Associate Director of the Cardiovascular Imaging Program and Director of Cardiac Computed Tomography at Brigham and Women’s Hospital. Audio editing by CardioNerds Academy Intern, student doctor Akiva Rosenzveig.
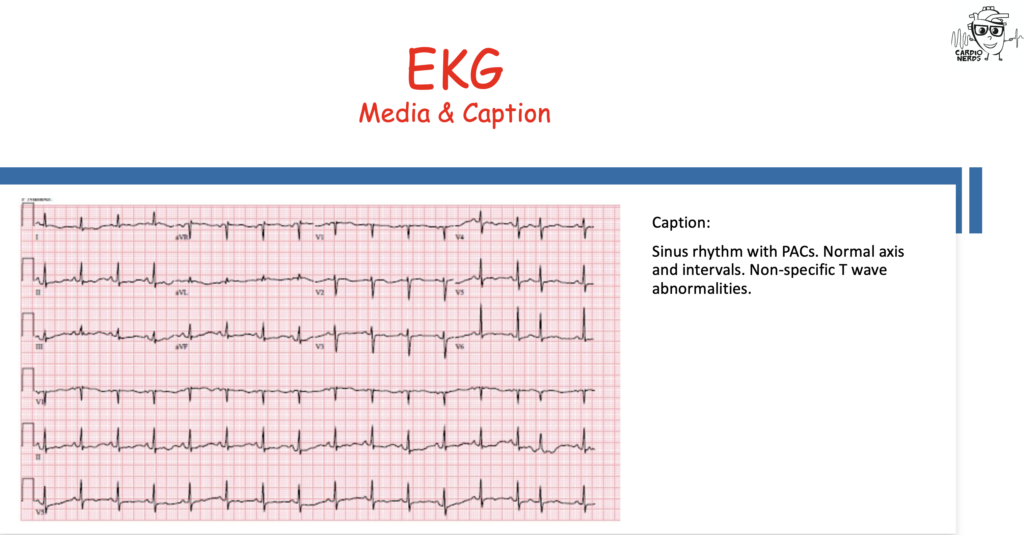
A 76-year-old man with a history of hyperlipidemia presented with one month of progressively worsening fatigue, weight loss, and dyspnea on exertion. Physical exam was notable for a 3/6 systolic murmur at the left upper sternal border, a flopping sound along the sternum heard throughout the cardiac cycle, and JVP elevated to the level of the mandible. TTE revealed a large heterogeneous echodensity in the right ventricular (RV) free wall that extended into the pericardium and into the RV myocardium with mobile components in the RV cavity and obstruction of the RV outflow tract. Nongated CT chest showed a solid nodule in the periphery of the left lower lung lobe. Gated cardiac CTA revealed a large heterogenous mass in the right atrioventricular groove that encased the proximal thoracic aorta and pulmonary artery and invaded the RV myocardium and RV outflow tract along with a large pericardial effusion. On cardiac MRI, the mass was isointense to the myocardium on T1-weighted images, hyperintense on T2-weighted images, and had heterogenous enhancement on late gadolinium enhancement images. Overall, the imaging findings were highly suspicious for cardiac lymphoma which was confirmed with biopsy of the lung nodule; pathology showed a large B cell lymphoma. The patient was treated with R-CHOP therapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), and TTE after 6 cycles of chemotherapy demonstrated resolution of the RV mass.
CardioNerds is collaborating with Radcliffe Cardiology and US Cardiology Review journal (USC) for a ‘call for cases’, with the intention to co-publish high impact cardiovascular case reports, subject to double-blind peer review. Case Reports that are accepted in USC journal and published as the version of record (VOR), will also be indexed in Scopus and the Directory of Open Access Journals (DOAJ).

Case Media
2. There is a large pericardial effusion, circumferential, measuring up to 2.2 cm adjacent to the right atrium and up to 2.3 cm anterior to the intraventricular septum. There is pericardial enhancement, indicative of pericardial inflammation.
3. This study was not optimized for the assessment of the coronary arteries. However, there are severe coronary artery calcifications. There is possible severe stenosis of the mid LAD.
4. Aneurysmal dilatation of the thoracic aorta, with measurements as reported in the narrative.
2. There is a large homogenous, soft-tissue intensity mass in the right atrioventricular groove infiltrating the right ventricle free wall and cranially extending anterior to the aorta and main pulmonary artery. The mass encases the main pulmonary artery, the aortic root, the right coronary artery, and the left main coronary artery. The mass invades the right ventricular outflow tract and proximal main pulmonary artery, resulting in severe luminal narrowing at the level of the RVOT/pulmonary artery valve. For the dimensions of the mass, please refer to cardiac CT from 12/1/2021. The mass is isointense to myocardium on T1-weighted images and hyperintense on T2-weighted images. The mass avidly enhances on first-pass perfusion images. There is heterogeneous enhancement of the mass on late gadolinium enhancement images.
3. There is a large circumferential pericardial effusion, measuring up to 2.3 cm.
2. Additional discrete mediastinal and hilar nodes, and left lower lobe nodule, most likely additional areas of lymphomatous involvement. Moderate uptake along right adrenal nodule may represent additional site of lymphomatous involvement
3. Small bilateral pleural effusions and small to moderate pericardial effusion.
Pearls – A Rare Cause Of Fatigue, Dyspnea, And Weight Loss In An Elderly Man – Brigham and Women’s Hospital
- In the diagnostic approach for cardiac masses, consider: 1) age of patient at time of presentation, 2) epidemiologic likelihood and clinical probability, 3) location of tumor, and 4) tissue characterization of the mass on CMR.
- CMR allows for better characterization of soft tissues and can assess mass morphology, dimensions, homogeneity, and infiltration into surrounding tissues.
- On CMR, cardiac lymphoma typically shows isointensity on T1 imaging and hyperintensity on T2 images.
- Cardiac CT allows for high spatial and temporal resolution, and can be useful to define cardiac masses that involve the coronary arteries; compared to CMR, cardiac CT has a greater ability to assess calcifications within a mass itself.
- Cardiac lymphomas have a predilection of right heart chambers, especially right atrium and can affect the AV groove, encasing the right coronary artery.
- Global systolic longitudinal myocardial strain on TTE is an indicator of early anthracycline-induced cardiomyopathy before overt reduction in ejection fraction.
Show Notes – A Rare Cause Of Fatigue, Dyspnea, And Weight Loss In An Elderly Man – Brigham and Women’s Hospital
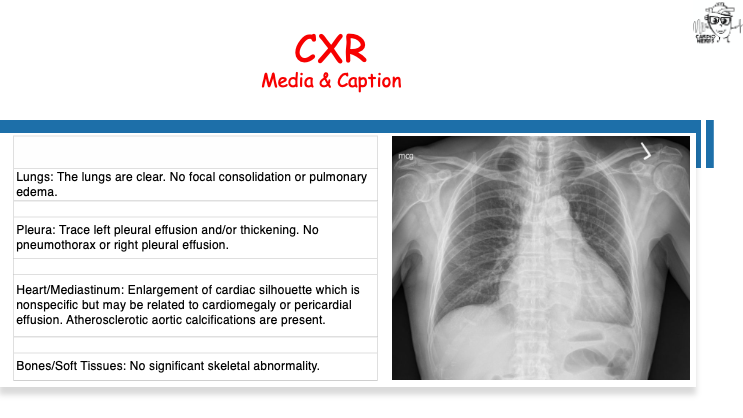
- What is the approach to an enlarged cardiac silhouette noted on chest x-ray?
- Cardiothoracic ratio of greater than 50%.
- Two possible “buckets” of diagnoses to consider are enlargement of heart related to cardiomegaly as opposed to a pericardial process like a pericardial effusion.
- For cardiomegaly, it can be from dilated or hypertrophic cardiomyopathy with most common causes including coronary artery disease, hypertension, valvular heart disease, and arrythmia-induced cardiomyopathy. Other buckets to consider are inflammatory causes, either infectious or autoimmune, as well as infiltrative diseases like amyloid or sarcoid, toxins (alcohol, cocaine, medications), endocrine, and nutritional causes (like a B1 or selenium deficiency).
- The most sensitive sign of a pericardial effusion on chest x-ray is enlargement of cardiac silhouette with a sensitivity of around 71%, but low specificity (1).
- With pericardial effusion, symmetric expansion of the heart contour leads to a globular appearance which is commonly referred to as flask-shaped or the water bottle sign (1).
- What is the approach to intracardiac masses?
- First, consider the age of the patient at the time of presentation since certain clinical entities like rhabdomyomas and fibromas are more common in the pediatric population (2).
- Second, consider the epidemiologic likelihood and clinical probability. In a patient with a recent anterior wall MI and akinetic ventricular apex, a cardiac mass on echo would raise concern for an intracardiac thrombus (2).
- Third, consider the location of the tumor. If the mass is on the valves, consider thrombus or a vegetation. While masses in the chambers can still represent thrombus, would also consider myxomas, lymphomas, and metastases (2).
- Fourth, consider the tissue characterization of the mass on further diagnostic imaging such as CMR (2).
- What is the role of multimodality imaging in the evaluation of intracardiac masses?
- TTE is the first modality utilized in evaluation of a cardiac mass. TEE is useful specifically when valvular lesions are suspected or in patients with atrial masses or with mobile valvular lesions. It can help to characterize size, morphology, attachment site, extension, and hemodynamic effects.
- CMR allows for better characterization of soft tissue and can assess mass morphology, dimensions, homogeneity, infiltration in surrounding tissues. These can all help differentiate different types of masses and whether a mass is benign or malignant. Signal characteristics gathered from T1, T2, early gadolinium enhancement, and late gadolinium enhancement sequences can further assess fatty infiltration, necrosis, hemorrhage, and vascularity within a mass (3, 4).
- Cardiac CT is another option and offers high spatial and temporal resolution, multiplanar image reconstruction capabilities, and fast acquisition times. The large field of view also allows for assessment of chest and lung tissue, vascular structures, and assessment for other masses in the chest. CT may also be more helpful in defining surgical approaches and assessing how masses may involve the coronary arteries and assess for coronary artery calcifications or obstructive coronary disease (4).
- FDG-PET is also another valuable imaging option which offers evaluation of metabolic activity of tumors. PET imaging can also help guide biopsy location, staging, and planning for cancer therapy.
- What are key features of Primary Cardiac Lymphoma?
- Diffuse large B-cell lymphoma is the most common subtype, though others like Burkitt lymphoma, low grade B –cell lymphoma, and T-cell lymphoma have also been described.
- They occur more commonly in immunocompromised individuals and in immunocompetent patients, only account for 1.3% of primary cardiac tumors
- Presenting symptoms are usually nonspecific. They may manifest as dysrhythmias like heart block, syncopal episodes, or even restrictive cardiomyopathy.
- Approximately 20% of patients may develop acute heart failure before other symptoms.
- On echocardiogram, these tumors appear homogeneous, with predilection of right heart chambers, especially right atrium. The AV groove can be affected, potentially encasing the right coronary artery (5).
- On CMR, tissue appears isointense on T1-weighted imaging. On T2-weighted imaging, lesions are mildly hyperintense due to diffuse edema (5).
- What are risk factors associated with anthracycline toxicity and what are strategies for preventing and monitoring for cardiotoxicity when anthracycline therapy is planned?
- Up to 35% of patients receiving anthracycline therapy develop some form of cardiotoxicity (6).
- The risk of developing anthracycline induced cardiotoxicity is directly proportional to the dose of anthracycline received, and after studies demonstrated HF incidence of 26% with doxorubicin dose of 550mg/m2 as compared to 5% with dose of 400mg/m2, efforts have been made to limit cumulative anthracycline doses to 400 to 450mg/m2. In addition, hypertension, DM, and obesity are all associated with increased risk (6).
- There are two primary prevention strategies: using cardioprotective agents, and aiming to reduce potency of the anthracyclines. For cardioprotection, dexrazoxane is an FDA-approved cardioprotective agent for anthracycline induced cardiotoxicity (7).
- TTE is the most common modality used for detection and monitoring of anthracycline toxicity on the heart. While LV dysfunction is most commonly detected, recent investigations suggest that RV function is also significantly affected by anthracycline toxicity (8).
- Global systolic longitudinal myocardial strain on TTE has also emerged as a reproducible indicator of early anthracycline-related myocardial dysfunction and future reduction in LVEF (9).
References – A Rare Cause Of Fatigue, Dyspnea, And Weight Loss In An Elderly Man – Brigham and Women’s Hospital
- https://www.acc.org/latest-in-cardiology/articles/2019/09/09/10/46/chest-radiograph-signs-suggestive-of-pericardial-disease
- Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, Manisty C, Westwood M, Ghosh AK, Guha A. Cardiac Tumors: JACC CardioOncology State-of-the-Art Review. JACC CardioOncol. 2020 Jun 16;2(2):293-
- Motwani M, Kidambi A, Herzog BA, Uddin A, Greenwood JP, Plein S. MR imaging of cardiac tumors and masses: a review of methods and clinical applications. Radiology. 2013 Jul;268(1):26-43.
- Lopez-Mattei JC, Lu Y. Multimodality Imaging in Cardiac Masses: To Standardize Recommendations, The Time Is Now! JACC Cardiovasc Imaging. 2020 Nov;13(11):2412-2414.
- Jeudy J, Kirsch J, Tavora F, Burke AP, Franks TJ, Mohammed TL, Frazier AA, Galvin JR. From the radiologic pathology archives: cardiac lymphoma: radiologic-pathologic correlation. Radiographics. 2012 Sep-Oct;32(5):1369-80.
- Henriksen PA. Anthracycline cardiotoxicity: an update on mechanisms, monitoring and prevention. Heart. 2018 Jun;104(12):971-977.
- Vejpongsa P, Yeh ET. Prevention of anthracycline-induced cardiotoxicity: challenges and opportunities. J Am Coll Cardiol. 2014 Sep 2;64(9):938-45
- Liu JE. Anthracycline-Induced Cardiotoxicity: Remembering the Forgotten Ventricle. JACC CardioOncol. 2020;2(1):23-25.
- Potter E, Marwick TH. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc Imaging. 2018 Feb;11(2 Pt 1):260-274.