This chapter explores the clinical evaluation of ICU-acquired weakness, emphasizing its distinction from pre-existing conditions and highlighting the critical factors influencing diagnosis and treatment. It reviews the implications of muscle and nerve injuries, risk factors, and the impact of ICU treatments on patient outcomes, including longer recovery times and increased mortality rates. The conversation further investigates the pathophysiology behind critical illness myopathy and neuropathy, underscoring the necessity of tailored management strategies for better rehabilitation.
Play episode from 12:06
chevron_right
Transcript
chevron_right
Transcript
Episode notes
Today we’re talking about a topic that is relevant for all critical care physicians but under-examined: ICU Acquired Weakness. We are joined by two excellent guests to walk through a case and discuss the diagnosis, pathophysiology, prevention, and treatment of ICU Acquired Weakness. Check out our associated infographics and key learning points below.
Meet Our Guests
Jim Devanney is a Physiatrist who just completed a neurocritical care fellowship at BIDMC. He is transitioning to a clinical associate position at University Health Network – University of Toronto where he will be working as a PM&R consultant within the ICU.
Kalaila Pais is a third year internal medicine resident at BIDMC, interested in pulmonary and critical care and medical education and is returning for her third Pulm PEEPs episode.
Key Learning Points
Definition & Clinical Presentation
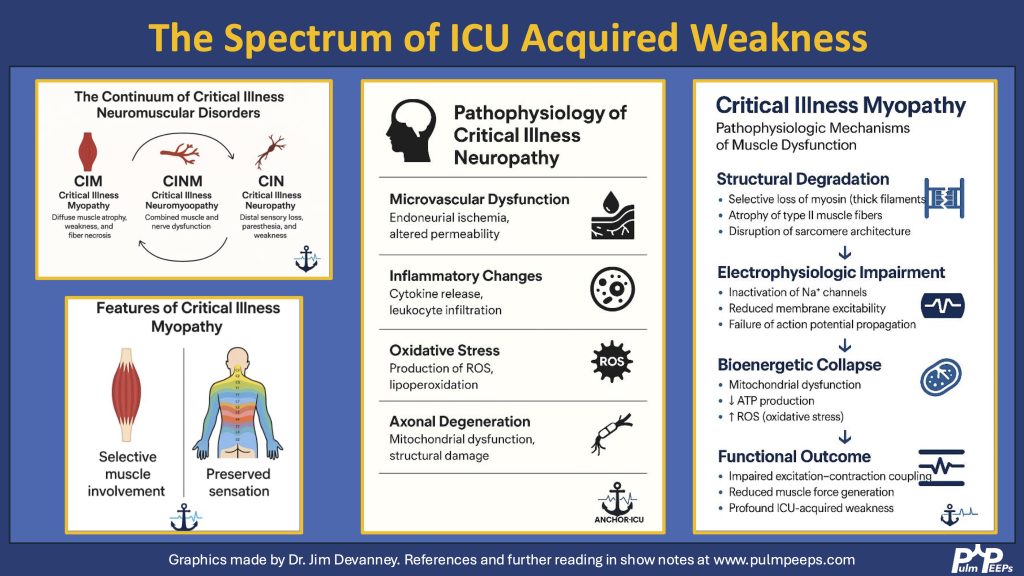
ICU-AW refers to new-onset, generalized muscle weakness that arises during critical illness, not explained by other causes.It typically presents as:
Symmetric, proximal > distal weaknessRespiratory muscle involvementPreserved cranial nerve functionNo sensory deficits in myopathy (sensory loss points toward neuropathy)
Differential Diagnosis Using Neuroanatomical ApproachAn anatomical approach (central → peripheral) helps localize the etiology weakness